Archive for the ‘science’ Category
J Allergy Clin Immunol. 2011 Feb;127(2):355-60.
Krefting Research Center, University of Gothenburg, Göteborg, Sweden.
Abstract
It is increasingly clear that asthma is a complex disease made up of number of disease variants with different underlying pathophysiologies. Limited knowledge of the mechanisms of these disease subgroups is possibly the greatest obstacle in understanding the causes of asthma and improving treatment and can explain the failure to identify consistent genetic and environmental correlations to asthma. Here we describe a hypothesis whereby the asthma syndrome is divided into distinct disease entities with specific mechanisms, which we have called “asthma endotypes.” An “endotype” is proposed to be a subtype of a condition defined by a distinct pathophysiological mechanism. Criteria for defining asthma endotypes on the basis of their phenotypes and putative pathophysiology are suggested. Using these criteria, we identify several proposed asthma endotypes and propose how these new definitions can be used in clinical study design and drug development to target existing and novel therapies to patients most likely to benefit. This PRACTALL (PRACtical ALLergy) consensus report was produced by experts from the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
PMID: 21281866
Today I read an article in the New York times describing the necessity to remove the American tradition of listing people as belonging to a “race”. Is race a genetic entity or a social structure?
Being a medical scientist, I am often exposed to research that is discussing medical findings related to the “race” which is denominated ”African American”. From a European perspective this is an incomprehensible term. What is “African American”? A term defining a person with dark skin living in America I presume? Looking for a definition, it seems that it is more a political or social term rather than something that is defined by genetic background. Well, perhaps partial Sub-Saharan African ancestry is required, which includes being a descendant from the slavery era, but also immigrants from African, Caribbean, Central American or South American nations are included in the definition. Thus, clearly the term “African American” is by definition involving a diverse group of people with fundamentally different genetic background. And from that perspective, individuals belonging to this “group” has very little genetically in common.
Therefore, I was so happy to see this article, because maybe it is time to start removing the conceptual thinking away from “race”, and start thinking about the “individual” as a unique entity where “race” is unimportant. The example of Ian Winchester, the partly Ghanian, partly Scottish, partly Norwegian mentioned in the article, illustrates very well that family history and cultural background is more important than “race”.
Medical research reporting differences in health outcomes in “African Americans” and “Whites” often imply differences in genetic background as explanations of different findings. That could of course be correct in some instances, but I would argue that differences in the social situation, health-related behaviour and health care utilisation, including health insurance access, are of much greater overall importance than small differences in genes and gene expression.
comments from NY times readers, most agreeing that race should become unimportant: http://nyti.ms/e6tE6k
I watched a really interesting lecture on the computer this morning, given by Ken Robinson (link at the bottom of this blog posting). It had been posted by Cezmi Akdis on his FB wall, and it is not only exceedingly interesting, but also witty and actually a “must see”.
It is discussing extensively about how the current educational systems are build around linearity, standard operating procedures and achieving pre-defined goals, without capturing the imagination, creativity and intuition of students. The lecture was passionate about finding models to develop schools to capture creativity in people, empowering them to develop new ideas and even new jobs.
But I think these concepts go way beyond our educational system, and capture the clash between on one hand “rules, regulation and standard operating procedures (SOP)”, and on the other hand “entrepreneurship, passion and invention, based on creativity and imagination”.
One example how today’s society has got it so wrong:
In our current time “invention” is a buzz word, which is related to “intellectual property (IP)” and “patents”. Those very closely connected terms have two processes connected to them that are based on totally and fundamentally different principles that contradict. Invention needs the lateral thinking and creativity of the inventor, but for the invention to have any value, society has built up a very complicated system of legal framework to protect patents and IP. The detail and structure by which patents can be legally claimed are exhaustive, complicated and to be honest, utterly boring for a creative inventor that eats and breathe lateral thinking and imagination, and from this spits out new ideas on a regular basis. For most inventors it would be impossible to sit down and author a document that requires very specific language and follows very specific SOPs. It is probably a contradiction in term.
Just think about the different personality traits of an inventor. He or she would most likely score high on personality traits such as “openness” and probably quite low on “conscientiousness” and “neuroticism”. On the other hand, a person that creates SOPs or legal framework, probably score very low on “openness” as they are prone to follow convention and rules, and very high on “conscientiousness”, for the same reason.
This contradiction in term, by which creativity is becoming packaged into boxes of limitation through the creation of regulation and SOPs in the workplace, is a key limitation of our current time. Here is a clip from Ken Robinson’s lecture:
http://www.youtube.com/watch?v=ySvbePkjEJo
Or check out the whole lecture, it is just over an hour long, but certainly worth the investment in time…
Sir Ken Robinson’s lecture at the Aspen Institute, >1h: http://fora.tv/2010/07/08/Sir_Ken_Robinson_The_Element
Gothenburg will bid for 2012 International Workshop on Exosomes (IWE), PLUS microvesicles – should the meeting have another name?
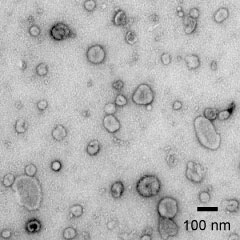
In the week after the very successful Exosome Meeting in Paris (http://www.curie.fr/fr/002348), there has been extensive discussion on how the community is captured and retains momentum and growth, a discussion that has been efficiently coordinated by Clotilde Thery. It was decided that the meeting will be held every year, and that a society is built, but not necessarily that a journal is developed. These are certainly wise decisions.t has also been suggested that the field of microvesicles will be incorported to the meeting next year, and we hope to engage the microvesicles community in achieving this. Would that mean that the meeting should have a complementary name, including the word “microvesicles”?
Personally I believe that a journal will come back on the agenda in due course. If the community of exosomologists doesn’t do it, someone else with a more commercial mindset might. Let’s give this thought another year and come back to it.
After careful reflection, the team in Gothenburg decided to develop a bid to hold the next exosome event in our city. We have identified and pre-booked a university hall that will take 350 people, that holds a large 60-poster exhibition area just outside the hall, and that can provide meals for all attendees at a reasonable price. If the meeting would become larger, we still have the opportunity to move to a professional congress centre in Gothenburg. We are putting together a short description on the bid, and it will be circulated to the community (=attendees at the Paris meeting) very soon for the final decision.
Gothenburg is a great city (http://goteborg.com/en/), just on the ocean, with a beautiful archipelago and nice walkable surroundings. The New York time has also named it one of the best non-capitals in Europe for restaurants, and you can read their praise of the city here http://bit.ly/gqSrrf .
Provisionally, the meeting date is April 18-21 in 2012. Put it in the agenda, and I will keep you updated on the progress. Expect final decisions within the next few weeks.
It is with sadness that EAACI is saying goodbye to its first Executive Director Silvia Schaller. Silvia has been instrumental at building up the EAACI Headquarters in Zurich in a very successful way, with a great group of professional staff dealing with all daily business such as educational activities, congresses and all of our communication platforms. Without Silvia, EAACI would not today be at the position it is. I wish to express my personal greatest gratitude to Silvia, and wish her the very best success in future adventures.
Is asthma one disease – probably not: It is multiple diseases each with different mechanisms
On the 2nd February, EAACI and AAAAI are publishing a “Rostrum” in the Journal of Allergy and Clinical Immunology, proposing that the subgroups of asthma should be called “endotypes”. The article outlines the arguments that asthma is a syndrome, consisting of several subgroups of disease. We are also proposing a series of subgroups of asthma that seem probable from a clinical perspective. This is the title of the publication:
Title: Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome Authors: Jan Lötvall MD, Cezmi A. Akdis MD, Leonard B. Bacharier MD, Leif Bjermer MD, Thomas B. Casale MD, Adnan Custovic MD, Robert F. Lemanske Jr.MD, Andrew J. Wardlaw MD, Sally E. Wenzel MD, Paul A. Greenberger MD.
Most likely, the paper will turn up on this page: http://jacionline.org/inpress
We chose the nomenclature based on an earlier publication, proposing the word “endotype” to explain the mechanism of diease http://en.wikipedia.org/wiki/Endotype .
Future research of understanding mechanisms of asthma should be based on presumed “endotypes” of asthma, instead of including any patient having symptoms of “the asthma syndrome”. Furthermore, novel treatments for asthma should probably be targeting subgroups of patients rather than any patients with typical asthma.
Severity of asthma may vary among endotypes. We have recently defined a population with clear signs of more severe disease, which we call Multi Symptom Asthma http://bit.ly/dJfsZ8. This is a distinct patient group, consisting of 2% of the whole population, and approximately 25% of all asthmatics. Is this severe asthma? Yes, because they express:
1) More symptoms of daytime asthma (not surprising)
2) More night time awakenings due to asthma
3) More asthma medication
4) Greater bronchial hyperresponsiveness, and
5) lower lung function
What are the risk factors of having severe asthma? Sinus problems, obesity (BMI>30), smoke and dust exposure… Regardless of asthma endotype!
We also believe lack of adherence to controller medication is a major risk factor, and evidence is emerging http://bit.ly/i56Xwd
Defining severe asthma – an impossible task? (or should we call it “difficult to treat”, “uncontrolled” or “exacerbation-prone” asthma????)
Severe asthma is difficult to define as is illustrated by a vast number of papers that have attempted to define this entity. Terms such as “steroid resistant asthma”, “uncontrolled asthma”, “exacerbation prone asthma” and “difficult to treat asthma” are closely related to severe asthma, and the terminology becomes even confusing to any clinician or scientist working in the field.
We have recently defined a population with clear signs of more severe disease, which we call Multi Symptom Asthma http://bit.ly/dJfsZ8. This is a distinct patient group, consisting of 2% of the whole population, and approximately 25% of all asthmatics. Is this severe asthma? Well, they have:
1) More symptoms of daytime asthma (not surprising)
2) More night time awakenings due to asthma
3) More asthma medication
4) Greater bronchial hyperresponsiveness, and
5) lower lung function
Is that severe asthma? I think so… This group of Multi Symptom Asthma is without doubt enriching severe patients…
What are the risk factors? Sinus problems, obesity (BMI>30), smoke and dust exposure… We also believe lack of adherence to controller medication is a major risk factor, and evidence is emerging http://bit.ly/i56Xwd
“Intuition”, “creativity” and “responsibility” are repressed by “standard operating procedures” (SOPs) – is “quality assurance” good for progress and success?
As the person being utmost responsible for the association EAACI, I participate and support processes of developing “Standard Operating Procedures” (SOPs). These are aimed at simplifying processes and explaining how the organization functions and operates, helping staff and new members in understanding what they are doing and why. A lingering question I am carrying in my mind is asking whether these SOPs are good or repressive, and whether the responsibility and accountability of an individual in their professional life is repressed by such documents.
Personally, I am of the opinion that intuition is very important in any major process of development. Intuition is defined as “thoughts and preferences that come to mind quickly and without much reflection”, and provides opinion and solutions that are sometimes difficult to justify intellectually. It has also been argued that intuition is closely related to with innovation and creativity in science. But how do you write an SOP on how to include intuition in decision processes? I don’t think it can be done.
Creativity is another aspect of work and development that is crucial. Perhaps creativity is easier to enforce, with activities such as “brainstorming”, defined as a “group creativity technique designed to generate a large number of ideas for the solution of a problem”. I was surprised to discover that brainstorming does not necessarily lead to higher numbers of ideas or higher quality of ideas than other types of idea generation, because it involves a group that can be repressed by social interactions. Still, it has been shown that brainstorming does enhance enjoyment of work and a feeling of being involved in decision making and progress.
I started to read some articles about “accountability” and “responsibility”, and my level of confusion increased even more. Basically, an SOP makes you “accountable” to lack of success, should you not follow this SOP. However, if you have followed the SOP and failure and lack of progress is the result, have you then been “responsible” in your actions?
Confusing? Yes, I know 🙂
Polosa and colleagues today published a paper in Respiratory Research, showing that those that smoke, and then develop asthma, develop a more severe form of disease http://bit.ly/eRi9W0. Basically, the investigators followed a substantial group of patients with allergic rhinitis (372 individuals) over ten years, as it is well known that these have higher risk of developing asthma. Indeed, smoking increased the risk of developing more severe disease, and the severity was closely related to amount of smoking. Basically, having smoked increased the risk about five times to have signs of more severe asthma, as described by the investigators: “Compared to 0 pack years, those who smoked 1-10 pack-years had an OR of 5.51(1.73-17.54) and those who smoked more than 10 pack-years had an OR of 13.38(4.57-39.19) to have uncontrolled asthma.”
The individuals with more than ten pack-years of cigarette smoking may of course have entered a phase of “mixed asthma and COPD”. Still, these data are compelling.
Another argument that tobacco for smoking should be totally banned
Crowdsourcing – the future of taking advanced decisions?
Crowdsourcing is a recent word that I have just picked up in the last week or so. It basically means that you ask “anyone” to help you with something. A project is allocated to an undefined, large group of people or community (a crowd), through an open call. Look at Wikipedia:
http://en.wikipedia.org/wiki/Crowdsourcing.
Actually, Wikipedia is probably the best example of crowdsourcing. Asking “anyone” to contribute, getting on average the best possible answer?
Will experts be redundant in the future? I don’t think so. They will be around. But they have to be able to master tasks such as “crowdsourcing” . In Wikipedia you can read “Crowdsourcing is a distributed problem-solving and production model. In the classic use of the term, problems are broadcast to an unknown group of solvers in the form of an open call for solutions. Users—also known as the crowd—typically form into online communities, and the crowd submits solutions. The crowd also sorts through the solutions, finding the best ones. These best solutions are then owned by the entity that broadcast the problem in the first place—the crowdsourcer—and the winning individuals in the crowd are sometimes rewarded.”
Can crowdsourcing be used to find solutions to problems in medicine? Can crowdsourcing help provide the best possible advice to patients. Can crowdsourcing be the future of progress?
What is a medical association but a “crowd”. Actually, it is a quite large crowd with very specific knowledge. In fact, EAACI is using crowdsourcing when we are planning congresses, by asking the membership to contribute. Every single member gets an e-mail and a possibility to suggest topics, speakers and symposia. And it works.